


Dues Structure Changes
As you are now aware, the Board of Directors approved and implemented a new dues structure for the calendar year 2014. In making this decision the Board carefully reviewed the dues of other similar organizations, alternative sources of revenue as well as organizational changes that have occurred since our last dues increase in 2009.
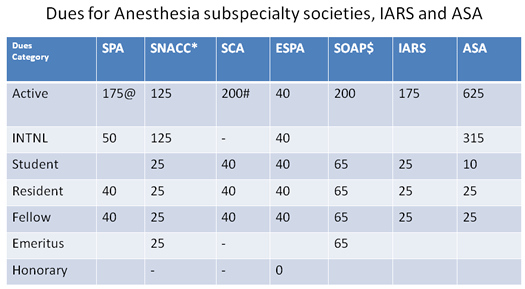
As the Treasurer I was asked several months ago to investigate dues of various similar organizations both US and abroad. I also reviewed the dues history of the organization and ultimately drafted a report that included recommendations to the board regarding future dues.
A copy of the comparison chart from that report is below:
The recommendations made were then carefully considered by the Board and the Boards of our member organizations such as CCAS. As we are not directly affiliated with the organizations that you mentioned in your note we are not privy to their plans for dues adjustment. It is unfortunate, but not surprising, that several organizations chose to increase dues at the same time. Many organizations like the SPA chose to limit dues increases during the recession, but as the economy began to improve they have decided to adjust dues and other fees such as registration to keep pace with their costs.
Please be assured that the SPA is responsive to its membership and takes its responsibility as good stewards of our dues income very seriously. I invite you to participate in the Society by attending any or all of our committee meeting including the finance committee. The dates and times of the meetings will be posted in the weeks prior to the next meeting.
If you would like to provide input directly to the board please feel free to contact me by e-mail (flick.randall@mayo.edu).
![]()
Thinking About Improving the Perioperative Experience
In his book, “Prescription for Excellence”, Joseph Michelli details how UCLA Health System morphed from an organization with poor patient satisfaction scores, despite outstanding clinical outcomes, to an organization “revered worldwide for its top tier patient/customer care”.
One chapter in particular strikes a chord for me as my department wrestles with ways to advance our hospital’s commitment to provide “family-centered care”. The chapter is titled “Delivering Exceptional Outcomes Here and Now” and commences with the following quote:
“Quality is never an accident;
It is always the result of high intention,
sincere effort, intelligent direction,
and skillful execution.”
-William Foster
The author proceeds to introduce the concept that success in business demands consideration for how consumers perceive the value of the product or service provided to them. This perception is determined by combining the perceived quality of the product or service with the perceived quality of the consumer experience and then subtracting the price paid.
Value = [perceived quality of product + perceived quality of service experience] – price
As physicians we focus our efforts on product quality. Reduce the risk for medication error, optimize postop analgesia, eliminate nausea and vomiting, prevent catheter associated blood stream infections, and so forth. This is the right focus and we should continue, even accelerate these efforts. Price is often less obvious to our patients as payments are often made through third-parties (private insurance, Medicaid, etc). Consequently, value for our families is often distilled to clinical outcome and the process of care.
Later today, I will join a small group of anesthesia colleagues to review survey data gathered from families undergoing surgery at our hospital. The survey asks families about pain management and nausea but also questions evidence for compassion, courtesy, teamwork, good communication and listening skills. For each question there is a rating as well as a coefficient describing that question’s correlation with the overall goal of improved family satisfaction.
As we dive into this data, we will look for areas where we as a department can improve and consequently impact our families’ perioperative experience. We hope to identify one worthwhile action that we can recommend for immediate implementation by our group.
One of the five principles for organizational success described by Mr Michelli is “make the best better”. That’s our focus here in Seattle as we look to elevate the perioperative experience for our families. If we succeed, the benefits to the institution as well as individually are tangible. According to Mr. Michelli, these include greater profitability, improved patient loyalty and positive staff morale, retention and recruitment. Entering 2014, that sounds like a prescription for excellence that gives me excitement for the year ahead.
With that said, this newsletter celebrates the humanitarian work of Dr. George Gregory, a legend of our field. He is a most worthy recipient of the ASA’s Nicholas M. Greene Outstanding Humanitarian Contribution Award. Reviews of our annual meeting held in San Francisco in October are included along with a pro-con debate of parental presence in the OR and a review of anesthesia-related dental injuries. These will prove interesting reads.
Enjoy!
![]()
Dr. Gregory Receives ASA's Nicholas M. Greene Outstanding Humanitarian Contribution Award
Maurice Zwass
UCSF Benioff Children’s Hospital
San Francisco, CA
Constance Monitto
Johns Hopkins University
Baltimore, MD
Dr. George Gregory, Professor Emeritus of Anesthesia at the University of California San Francisco, was presented with the American Society of Anesthesiologists’ Nicholas M. Greene Outstanding Humanitarian Contribution Award honoring his longstanding involvement with organizations such as ReSurge International which provides free reconstructive surgery for the poor in developing countries.
Dr. George Gregory
Dr. Gregory, who received the award at the ASA’s annual meeting in San Francisco in October, is a true pioneer in pediatric anesthesia. He is internationally known for his many academic accomplishments, including his groundbreaking description of continuous positive airway pressure (CPAP) in neonates and infants and his textbook of Pediatric Anesthesia, now in its fifth edition.
In addition, working with groups like ReSurge International (formerly Interplast), where he is director of anesthesia, he has helped to teach surgeons, anesthesiologists, and nurses working around the world to care for patients with burns and craniofacial defects, thereby providing ongoing medical access to reconstructive surgery and follow-up care in underserved areas.
According to Dr. Gregory, “there are millions of children and adults throughout the world who have little or no access to health care, especially surgery to correct cleft lips and palates or the aftermath of burns. Burns are common, but the victims are often unable to get adequate early burn care and are left with contractures that prevent them from using their hands, arms, legs, or extending their necks. The only way they can get treatment for contractures is when groups such as ReSurge . . . go to the site and correct these abnormal conditions.”
It became apparent to Dr. Gregory, though, that in many of the countries served, anesthesia was provided by technicians who had only one or two years of anesthesia training following high school. These anesthesia providers often simply wanted to know how to set the knobs on the anesthesia machine and how much of each drug to give without any consideration of the patient’s illness or condition, factors that at times play a role in the very high perioperative mortality rates (as high as 1:50 cases) seen in some parts of the world.
“It has been my goal to develop ways to improve education for people in the countries we serve. This usually begins by finding an anesthesiologist or other persons who are responsible for education of anesthetists and to involve the educator in the development of programs that will allow the local anesthesia providers to provide physiologic and pharmacologic based anesthesia.”
To promote education, he has been involved in organizing conferences for international providers and educators and helping defray costs to allow attendance. “By providing this education and educational materials, we have shown them new ways to think about anesthesia, which we hope will be taken back to their communities to educate others.”
To further address these issues, Dr. Gregory and colleagues are in the midst of writing and editing a Pediatric Anesthesia e-textbook that will be housed at the Society for Pediatric Anesthesia website and will be available free of charge to anyone from developing countries who wishes to download it.
In our global environment, some anesthesia providers cannot afford textbooks or journals, but they often have access to a computer and the internet. He is hopeful that this book “will meet a largely unfulfilled need. As we go forward, our goal is to establish a website where anesthesia providers in developing countries who have questions about anesthesia can send their questions to the site and members of the Society of Pediatric Anesthesia can answer their questions with information that is appropriate for a developing country.”
![]()
SPA & ASA Annual Meeting Reviews
SPA Meeting Reviews
Session I: Clinical Care of the Neonate
Moderator: Peter Davis MD, FAAP
By Elizabeth S. Yun, MD
University of Wisconsin School of Medicine
Madison, WI
The first session, Clinical Care of the Neonate, reviewed various clinical issues associated with neonates and premature infants and was moderated by Dr. Peter Davis (University of Pittsburgh).
The first speaker, Dr. Hannah Glass (University of California, San Francisco), gave a lecture on Newborn Brain Injury: Imaging, Therapies and the Future. She noted that brain injury in the neonate is a common problem. The initial diagnosis is made by observing clinical signs of encephalopathy and using bedside EEG. For a more in depth study of the brain, the MRI provides the highest quality image despite the challenges of safety and small head size. These MRI images provide important information about the rapid brain development in a neonate. Dr. Glass then discussed different types of brain injury in the premature and full term neonate.

Hannah Glass, MD
In the premature baby, the brain injury mechanism involves the white matter. Based on gestational age the neonate brain undergoes several important developmental changes. One is the formation of oligodendrocytes, the cells involved in myelin sheath production, and another is the activity and regulation of antioxidants that detoxify free radicals. Both mechanisms are vulnerable to insults that occur in the developing premature brain. Imaging now shows that the white matter injury is predominantly focal and noncystic. It appears that this damage is due to postnatal events and not the gestational age of the child and appropriate ventilation to prevent insult may improve white matte injury.
The importance of preventing white matter injury is highlighted by the increased incidence of cerebral palsy and long term cognitive problems in the patients who survived prematurity. She then reviewed neurologic injury in the term neonate. The predominant injury is hypoxic ischemic encephalopathy due to asphyxia from a birth trauma. Unlike the premature infant, the damage is located in the deep gray matter of the thalamus and the basal ganglia, the most metabolically active part of the brain. Another location is the watershed intervascular zone.
Treatment for these patients includes therapeutic hypothermia, both selective head and whole body cooling. While this therapy improves survival and disability, about 50% of patients do not experience this benefit. Another common neurologic problem for term neonates is stroke. MRI imaging demonstrates disrupted connections within the brain in both the acute and chronic phase. While forty percent of patients are normal, about fifty seven percent will suffer motor and cognitive abnormalities.
Dr. Glass then briefly reviewed the effects of congenital heart disease and the developing brain. MRI imaging suggests that a term infant with CHD shares characteristics with the premature brain. The injury though appears to occur before surgical correction as well as after.
Finally, Dr. Glass suggested some new approaches to neuroprotection such as optimizing the timing and depth of hypothermia and new agents that may prevent damage at different stages of brain development.
The second lecture, Perioperative Care of HFOV & ECMO in the NICU, by Dr. Stephen Stayer (Baylor College of Medicine), reviewed the use of high frequency oscillatory ventilation (HFOV) and ECMO for neonates with respiratory and cardiac failure. Premature infants’ lungs have poor mechanics at birth.
They have a deficiency of surfactant production, reduced lung volumes, compliant chest wall, and fluid filled saccules, predisposing the lung to injury. The previous conventional ventilation strategy of tidal recruitment and derecruitment caused lung volutrauma in these patients. In response, an open lung concept is now used, involving just enough pressure to produce a tidal volume 3-5 ml/kg and PEEP to maintain recruitment with minimal damage to the premature lung.
The mechanics of HFOV fit these needs and therefore is used in patients in severe respiratory failure. It uses a diaphragm that drives gas during both inspiration and expiration with extremely small tidal volumes. Rates are set at 3.5-15 hertz and are equal to 210-900 breaths per minute. Mean airway pressure acts as PEEP to maintain lung distension and is adjusted for oxygenation. With this ventilation mode, alveoli stay open continuously. While HFOV has improved survival and outcomes in animal models, the human outcomes are less positive.
Dr. Stayer then reviewed anesthetic considerations for patient on HFOV. Initiation of HFOV is associated with a drop in blood pressure because the increase in intrathoracic pressure can decrease cardiac output and preload. Many surgical procedures can be performed while the patient is still on HFOV since conversion from HFOV can be poorly tolerated due to worsening gas exchange. To increase ventilation, the delta P is increased to adjust tidal volume and the rate is decreased to improve CO2. The end tidal CO2 is not measured. Kinks in the circuit must be avoided. If there is a disconnection in the circuit, the ventilator powers down and needs to be powered up when reconnected.
Dr. Stayer next discussed ECMO. He reviewed history of its use and noted that while use for pulmonary indications has plateaued because of alternative strategies like HFOV, its use for cardiac rescue and congenital heart disease has increased. The overall survival is 85% with 94% for patients with meconium aspiration syndrome and 55% for patients with CDH. Classic contraindications for ECMO include estimated gestational age less than 34 weeks, grade 3 intraventricular hemorrhage (IVH), cardiac arrest, and conditions incompatible for meaningful life.
Due to modifications in ECM, these contraindications are now being challenged. The modern ECMO circuit has a built in heater cooler system, hollow fiber oxygenators that have less flow resistance, use of smaller priming volumes, centrifugal pump that causes less trauma to blood cells and the use of veno-venous cannula. Anesthetic considerations include awareness of blood loss due to the anticoagulation needed to maintain the circuit, the need for adequate venous access for transfusion, the dependence of VV-ECMO on the patient’s native cardiac output and the limited access to the patient. A perfusionist should be present to help manage the circuit.
Dr. Andrew Costarino (A.I. DuPont Hospital for Children) gave the third lecture, Outcomes of the Extremely Premature Neonate. He described the survival outcomes and selected morbidities of this patient population. As per CDC data from 2011, preterm births make up 11.7 % of all births with those under 28 weeks gestation accounting for 0.7% of those births.
Overall, the preterm birth rate is going down although it still is increasing in Hispanic and African American populations. Along with the decrease in preterm birth was a decrease in the frequency in multiple gestations, a common reason for preterm births. He noted that data from the NICHD neonatal network showed improved in mortality as gestational age increased by one week and the weight increased by 100 grams. These improved outcomes are due to changes in therapies including antenatal steroids, surfactant, and targeted oxygen therapy.
By pooling the data from multiple large population studies over the years, he looked at various outcomes based on gestational age. He defined viability as the age of 50% survival and noted that it is now at 23-24 weeks gestation. He then discussed various morbidity outcomes for the extreme premature infant. Historically, the development of retinopathy of prematurity (ROP) was linked to the high FiO2 used in preterm infants to prevent apnea. However the low FiO2 needed to reduce the incidence of ROP was associated with increased mortality and NEC.
In response, several studies determined that the target oxygen saturation of greater than 90% was the best for these infants. Another long term morbidity concern for the extremely premature infant was neurodevelopmental disabilities in the five domains of motor, cognition, speech and language, social, and activities of daily living. He focused on motor outcomes, specifically cerebral palsy. Cerebral palsy (CP) is a nonprogressive motor disability due to damage of the motor control centers of the brain. Premature infants are at a higher risk for cerebral palsy and it is often used as a marker for over all neurologic outcomes of prematurity.
While the risk appears to be decreasing, the better survival at younger ages may be associated with increased morbidity. Risk factors for CP development include periventricular leukomalacia (PVL), grade 3-4 IVH, bronchopulmonary dysplasia (BPD), male gender and postnatal steroids. Another concerning morbidity is severe cognitive delay as measured on the Bayley Infant Dvelopmental scale that takes a raw score based on behavior/play and converts it a composite scale. One part measures language and cognition and the other looks at motor skills. Risk factors for this delay are similar to CP risk factors including male gender, PVL, IVH. However, all these neurodevelopmental issues overlap.
In summary, premature births are a significant course of infant mortality and morbidity with the smallest infants having 30-50% mortality and survivors having 40-80% risk of significant morbidity. Factors improving survival include new ventilation strategies, a target O2 sat > 90%, antenatal steroids. The ultimate goal is hospital discharge around the child’s EDC if there are few complications and to follow for long term learning, behavioral and social problems
The final speaker of this session, Dr. Clare Brett (University of California, San Francisco), presented Care of the Formerly Premature Pediatric Patient. She reviewed the long term consequences of prematurity including the effects on chronic lung disease and development. She noted that prematurity is a life long diagnosis since issues in this stage can affect adult disease.
As previously discussed, survival without morbidity increases with increases in gestational age and extremely premature infants are at risks of significant morbidity. She focused on two outcomes of most interest in these patients, respiratory and neurological. The unifying theory for the outcomes in both organ systems is events in utero that prime the patient for increased susceptibility for postnatal insults such as oxidative stress, infection, ischemia/reperfusion. These insults lead to inhibition of growth and development in these organ systems with long term consequences.
She first addressed respiratory outcomes. Recent studies show that prematurity is associated with a broad spectrum of symptoms and lung abnormalities lasting into adulthood. Bronchopulmonary dysplasia (BPD) is a chronic lung disease of the preterm. In the past “old” BPD occurred in the older premature infant. These patient’s lungs consisted of airway inflammation and fibrosis.
These days, “new” BPD occurs in the extremely premature infant exposed to surfactant. This new BPD is characterized by a disruption of alveolar development that may be due to a genetic susceptibility that may involve disruption v-endothelial growth factor leading to decreased alveolization and angiogenesis. The end result is smaller number of large alveoli. Both types of BPD have similar long term outcomes. Despite changes in therapy, the oxidative stress of premature birth at any gestational age contributes to the poor outcomes. Both types will present later in life with increased expiratory flow abnormalities, airway hyperreactivity and exercise induces wheezing that is partially reversed with bronchodilators.
A cardiovascular complication of BPD is pulmonary hypertension. This combination is associated with increased mortality and morbidity. The pathology is unclear although there may be fetal growth restriction due to placental insuffiency. More work needs to done to detect, monitor and treat pulmonary vascular disease to improve this outcome. The overall strategy for managing these patients is to evaluate for signs of exercise tolerance, reactive airway disease, and response to medications preoperatively and to prepare for airway hyperreactivity and bronchospasm perioperatively even in the asymptomatic patient.
As for neurological outcomes, despite improvements in managing the extremely premature infants, the rates of neurodevelopmental problems remain high. While neurosensory deficit rates improved, patients experienced deficits in speech and language, executive function, behavior problems, lower IQ. While preterm birth itself does not injure the brain, insults that occur after the birth damage the developing brain and may contribute to these issues.
White matter and gray matter volumes increase drastically in the third trimester making this period a critical time for brain development. Injury due to ischemia/ reperfusion, infection, inflammation to both white and gray matter leads to complex cascade that disrupts the coordinated growth of the entire brain. These structural abnormalities can persist into late adolescent and adulthood and cause poor cognitive and behavioral outcomes.
The implications for perioperative care include a variable response to sedative and anesthetic agents, postoperative pain control and premedication. Based on this research, the developmental reprogramming that occurs during the neonatal period has consequences that affect the child’s perioperative care for the rest of their lives. Future goals include creating new treatment and therapies to prevent damage in the early stages of life for these patients.
Session II: Perioperative Communication with the NICU
Moderator: James J. Fehr, MD
By Zulfiqar Ahmed, MD, FAAP
Anesthesia Associates of Ann Arbor
Ann Arbor, MI
The second session of the day was focused on peri-Operative communication between anesthesiologists and neonatal intensive care staff and was moderated by Dr. James Fehr (St Louis Children’s Hospital).
The first speaker, Dr. Shilpa Verma (Seattle Children’s Hospital) provided an overview of the subject. She successfully identified perioperative communication failures in the neonate, discussed patient safety concerns related to perioperative communication failure, and described strategies to improve perioperative communication.
Dr. Verma referenced the 1999 IOM report which states 44,000-98,000 people die each year as a result of preventable medical errors. In addition, Joint Commission (JCAHO) identifies poor communication as the root cause of almost 70% sentinel events, medical mistakes, and “near misses.” Dr. Verma went on to give a couple of examples where poor communication between NICU and anesthesia teams might occur.
Upon surveying NICU and operating room staff at Seattle Children’s Hospital, preoperative handoffs emerged as a common source for communication gaps. She went on to discuss specific deficiencies of the preoperative handoff (NICU to Anesthesia) that were identified. Preoperatively, the Anesthesia team received handoff from one person – the bedside RN. Doctor to doctor communication was lacking. The big picture, treatment goals, management challenges, airway concerns, social issues were missed; even an opportunity to communicate the anesthesia plan, intraoperative concerns and postoperative expectations was lacking.
To avoid these deficiencies, an ideal pre and postoperative handoff should involve key members of both teams (attendings, nurses, respiratory therapist) together in one room at the same time, talking to each other and exchanging critical information. After all, the moment the patient leaves the NICU, the anesthesiologist takes on the role of neonatologist, the respiratory therapist and the bedside RN. Hence, everyone’s presence during the handoff is critical.
According to Dr. Verma, a good handoff tool is:
- Standardized with respect to the people present, the tool used, the content and the language used.
- Includes an opportunity to ask questions, clarify and voice concerns.
- Identifies a handoff facilitator that owns the tool and is responsible for its completion
- Completed with all key members present (pre and postoperatively)
For successful implementation of any new method, their needs to be a culture change. Culture change begins with buy-in. Members from both departments must realize that failure in communication may cause harm to not only patients, but staff and institution as well. Leadership backing is fundamental – clinical directors, department heads, chief medical officer and nursing leaders help set the expectations. Finally, the process needs to be made easy.
The remaining two sessions were combined with two speakers from Children’s Hospital of Philadelphia sharing one presentation. The topic was “One Center’s Journey - Anesthesiology Perspective (John J. McCloskey, MD) and Neonatology Perspective (Natalie E. Rintoul, MD)”.

Natalie E. Rintoul, MD and John J. McCloskey, MD from
Children’s Hospital of Philadelphia
Several years ago, significant perioperative issues with neonatal surgical patients including poor staff communication, perioperative hypothermia, fluid shifts, coagulopathies, infections and inadequate pain management were identified at CHOP. These missteps resulted in adverse outcomes for some patients. The tremendous number of providers from various departments (NICU, anesthesia, nine divisions of surgery) and multiple provider levels (attendings, fellows, residents, CRNAs, nurse practitioners, and RNs) contributed to these issues. A multidisciplinary neonatal perioperative committee formed to address these issues developed guidelines, perioperative newborn/infant pathways and order sets aimed at improving perioperative outcomes.
A perioperative surgical checklist developed by this committee was displayed and discussed. One important part of the form includes discussion of the post-operative respiratory plan. Another outcome of this group was identification of neonatal surgical procedures that should be performed in the NICU. These included patients less then 1000 grams as well as those requiring HFOV, pressors or nitric oxide. CDH repairs and omphalocele tightening procedures also qualified.
Ongoing quality improvement projects arising from this committee include perioperative audits of reintubation, arrest, apnea, sepsis, central line infection and central line malfunction/loss rates. Also included was whether these rates differ by surgical specialty, timing (day versus night, weekday versus weekend/holiday) or location (OR versus ICU).
The session ended with an active question and answer session.
Thanks to Dr. Stephanie Wade of Anesthesia Associates of Ann Arbor for her help in editorial service.
Session III: Neonatal Simulation
By Jorge Gálvez, MD
Assistant Professor of Anesthesiology & Critical Care
The Children’s Hospital of Philadelphia
University of Pennsylvania, Perelman School of Medicine
Philadelphia, PA
The session on Neonatal Case Simulation was well attended with over 100 attendees. The primary goal was to introduce the use of trigger videos to assist in simulation and training for education programs. A trigger video is a short video clip, approximately 3 minutes long, which highlights a specific process. The video serves as an introduction to a discussion and can stimulate discussion by allowing analysis of specific events as well as stimulating the audience to remember specific situations where the problems highlighted played a role. The presenters focused on scenarios that involved team dynamics and communication including: transfer of care to NICU, induction of anesthesia and personnel management during a crisis.
Trigger videos are not new concepts. They have the benefits of stimulating a conference or teaching discussion. One of the primary values is that they are short and high yield. Instructors can highlight different parts by using the stop-rewind-replay technique to review specific points. Additionally they provide a rich opportunity for case, exploration, instruction and discussion. The trigger videos also have the benefit of allowing individuals from different disciplines to appreciate concerns and different subspecialty perspectives.
The presenters also discussed the process to make the trigger videos that were used in the presentation. The teams used 2 handheld Sony video camcorders, 2 tripods, 1 microphone and a simulation center. One of the videos also used a first-person point of view camera. These cameras are increasingly popular and affordable and allow the individual to wear it on their head. The video captured gives the viewer the perspective of the wearer. These cameras were particularly effective at demonstrating the perspective of the attending anesthesiologist during a crisis scenario.
The clinical scenarios presented were as follows:
Scenario I
An unscripted video that evaluated team dynamics and aspects surrounding sign-out from the NICU for an ex-24 week patient being evaluated for potential extubation now scheduled for a bronchoscopy and laryngoscopy. The video was based in the operating room and showed a resident setting up for a case that they were not familiar with. The attending assigned to the case appeared pre-occupied with running the Operating Room schedule and was not very helpful to the resident. The resident was attempting to communicate with the neonatologist, but was not able to contact the patients’ team when the patient suddenly arrived in the OR with the nurse transport team, who is also not very familiar with the patient. They do provide additional details about the patient: she had failed an extubation trial 3 days prior due to stridor and was treated with steroids. The fellow attempted to intubate unsuccessfully, and had to be intubated by the attending, but no information was provided about difficulty of the laryngoscopy and intubation. Over 50% of the audience answered that they have been in a similar situation before.
At Boston Children’s a pre-intervention survey demonstrated that sign-out was adequately performed 50% of the time. As a result, they developed a sign-out tool called: STICK: Serious issues, Twenty-four hour events, ICU team concerns, Concerns of the family, Knockout plan (anesthesia) and post-op care. After an education and implementation intervention, the handoff performance improved to 85%, but can still benefit from policy enforcement.
Scenario II
The second trigger video focused on communication during a procedure. There was an infant in the operating room that had an acute change in status. The end-tidal CO2 waveform disappeared. There were various individuals trying to figure out the problem at the same time: the resident was attempting to untangle the breathing circuit while the attendings were looking for suction. The resident was attempting to communicate a problem to the attending but was not heard. As a result of the miscommunication, the patient began to deteriorate before the team members began to work together to solve the problem.
The audience was then asked about speaking up, to which 15% of the audience said that they had been in situations where they felt that they should speak up but did not. The presenters highlighted that speaking up is a universal challenge, even though it could be important for patient safety. The reasons for not speaking up are often around fear of embarrassment or retribution. The framework for silence was outlined:
- Status differences
- Fear of damaging relationships
- Loss of trust, respect, or acceptance support
- Fear of futility (speaking up will not make a difference)
- Lack of experience in current job position
- Concerns about negative impact on others (not wanting to embarrass or upset someone, or get them in trouble)
- Poor relationship with staff
They advocated a strategy to build an environment that helps people feel comfortable and supported when speaking up. A NASA study showed the two-challenge rule works, in other words, speak up twice. In a cockpit, the strategy is that if you speak up and are unsuccessful, then you take over the controls. The adaptation for medicine is that if unsuccessful, you can call for help.
Another strategy is to use advocacy or curiosity to speak up. A simple statement of an observation or fact can stimulate a discussion. The individual can also attempt to find the other’s frame of reasoning. At the Center for Medical Simulation in Boston, residents are being trained with the two-challenge rule in a simulation approach (http://www.ncbi.nlm.nih.gov/pubmed/19444045). In this study, 40 residents went through a case simulation. They were then trained on how to speak up and underwent a second simulation. The results report that trainees felt empowered to speak up about patient safety.
Scenario III
The concept of Crisis Resource Management, which is an adaptation of the system developed for managing critical events in the flight industry known as Crew Resource Management was discussed. The simulations highlighted specific problems that can occur in the healthcare setting and discussed strategies to overcome these. This concept was demonstrated with a trigger video of a patient transport from the OR to the NICU. In this scenario, the patient had a critical airway and the anesthesia team was attempting to sign out to the NICU team. The NICU fellow appeared in a rush because of other ongoing emergencies. The attending anesthesiologist established ground rules by saying: “if you have to go, I understand. I’m happy to stay here and wait you're your attending because this baby has a critical airway.”
The session highlighted key steps to effective communication during handoffs, including:
- Shared situational awareness
- Ensure two-way communication
- Face-to-face handoff
- Clearly outline transfer of patient responsibility
- Provide support (mutual performance monitoring)
- Provide information and structure
- Use checklists (example: Stanford iPass) to transfer care from OR to NICU
The presenters applied the various error theories including cognitive error, premature closure, commission bias, overconfidence bias and fixation bias to the elements in the trigger video. It was a skillful demonstration of the stop-rewind-replay techniques to stimulate discussion. The challenging scenario involved the child with the critical airway having an acute desaturation when transitioning to the NICU ventilator and re-taping the tube. The NICU fellow was adamant that the tube had come out and wanted to remove the tube and mask ventilate the child. The attending anesthesiologist did not support that plan and continued to assess the child and found that the ETT was too deep. Upon withdrawing the ETT slightly, the situation resolved. In this case, the RN begins to suction the patient, who then goes bradycardic and hypoxic. The care team focuses on the monitor while making decisions but oversees the fact that the patient is not being ventilated and the circuit is disconnected due to the suctioning.
The discussion focused on hazardous attitudes that can cloud judgment, including anti-authority, macho and invulnerability. Berner et al. (http://www.ncbi.nlm.nih.gov/pubmed/18440350) showed that overconfidence in medicine led to diagnostic errors, and residents tend to stay committed to an incorrect diagnosis even if presented with data that indicates they may be incorrect.
Lastly, the dual based theory was discussed. This highlights that there are two main systems for decision-making. The first system relies on intuitive and subconscious thinking while the second system relies on analytic and conscious thinking. Clinicians of varying experience levels may rely on one system more than the other. Specifically, Sibbald reviewed the performance of novice, intermediate and expert clinicians in ECG interpretation and found that expert clinicians were more likely to alternate between the two systems of reasoning (http://www.ncbi.nlm.nih.gov/pubmed/23625338). In this setting, both novice and expert clinicians were able to use the checklists effectively, but often the checklists caused a greater cognitive load on expert clinicians while the novice clinicians demonstrated a greater benefit from using the checklist.
The panel members produced all the videos shown during the session. They required equipment that is relatively accessible in most operating rooms. By and large, the essential equipment is a mannequin/doll, medical equipment (monitor, support lines), a video camera such as a smartphone and a computer for editing. Some of the videos shown were produced in a 2-hour film session with intermittent editing over two months.
The discussion then focused on educational interventions to assist anesthesiolologists and trainees in managing difficult transitions of care or emergency situations. All presenters applied trigger videos to stimulate and guide discussions on the topic. The main benefit of trigger videos is that after they are made, they can be stored in a permanent library and are available for individual or group use any time.
Session IV: Medical Marijuana Use for Pediatric Pain
Moderator: Constance Monitto, MD
By Karen Dean, MD
Children’s Hospital Colorado
University of Colorado School of Medicine
Denver, CO
This year’s fall meeting wrapped up with an engaging pro/con debate on the merits of medical marijuana, with Stephen C. Brown, MD (Hospital for Sick Children) articulating the benefits of medical marijuana use and Jeffrey Galinkin, MD, FAAP (Children’s Hospital Colorado) voicing the pitfalls.

Stephen C. Brown, MD
The discussion is timely, with Canada and 20 US states now having passed laws to legalize medical cannabis (Alaska, Arizona, California, Colorado, Connecticut, Delaware, Hawaii, Illinois, Maine, Massachusetts, Michigan, Montana, Nevada, New Hampshire, New Jersey, New Mexico, Oregon, Rhode Island, Vermont, Washington, District of Columbia), and more states likely to follow suit.
Hopefully not surprisingly, no one was willing to make the true “pro” argument in favor of children smoking pot. What Dr. Brown did give us in his talk was a thoughtful overview of the current evidence for synthetic cannabinoids and their potential applications in the pediatric pain population. He began with a historical overview, describing medicinal use of marijuana across the world as far back as ten thousand years ago, and ending with current practice. The marijuana plant contains over 400 chemical compounds, approximately 85 of which are cannabinoids. These cannabinoids and their synthetic derivatives act at CB1 and CB2 receptors to modulate pain processing and anti-inflammatory activity.
Dr. Brown shared the results of several adult clinical trials with cannabinoids, including two key reviews of multiple randomized controlled trials by Campbell et al. (BMJ 2001) and Lynch et al. (Br J Clin Pharmacol 2011). To date, studies have demonstrated poor efficacy in the treatment of acute pain, especially postoperative pain. Data with chronic pain are more promising, with some evidence of reduced pain intensity in patients with a multitude of chronic pain conditions.
Unfortunately, there is a paucity of evidence for cannabinoid use in children, which boils down to one dated trial of nabilone as an anti-emetic, and a case report of dronabinol use in two adolescents with neuropathic pain. While the idea of medical cannabinoid use has potential, much more research is needed first.
For the “con” argument, Dr. Galinkin focused his comments on the most common mode of medical marijuana use, which is smoked cannabis. The list of reasons to avoid the leafy substance is long. First of all, efficacy data is extremely limited and is likely to remain so. This is largely because marijuana is a Schedule 1 drug, and the FDA is unlikely to approve efficacy research for a drug the DEA deems to have high abuse potential and no currently accepted medical use. Also, there is no “standard” marijuana, with each plant varying in potency and purity, making research challenging.
Dr. Galinkin then turned his attention to the adverse consequence of medical marijuana. Adolescent marijuana trend data is alarming (see www.monitoringthefuture.org), and marijuana addiction is a growing problem. Over 60% of adolescents entering drug treatment centers identify marijuana as their number one drug of choice. Rates of diversion are high, with one study reporting 74% of adolescents in drug treatment centers acquiring medical marijuana from registered users. Marijuana toxicity in children, once unheard of, is now becoming a reality in emergency rooms. There has also been a parallel increase of toxic exposures in pets. And who can blame them, when companies are putting out marijuana-laced baked goods, cotton candy, and caramel corn?
Perhaps most frightening though are the potential long-term neurocognitive effects of marijuana use. Adolescent marijuana-users routinely test poorly in tasks that require working memory, visual scanning, cognitive flexibility, and learning. The level of cognitive impairment is proportional to the frequency of drug exposure. There is also an emerging connection between marijuana and early psychosis and schizophrenia.
The carcinogenic potential of cannabis is also of concern. Smoked marijuana is the ultimate “dirty” drug, containing hundreds of chemical compounds and contaminated with pesticides, heavy metals and fungal spores. The average joint has 50% more carcinogens and 300% more tar than a tobacco cigarette. One cohort study reported a two-fold increase in lung cancer among heavy marijuana smokers.
One of the best highlights of the talk was watching a video of habitual marijuana users trying to navigate a vehicle test course with increasing blood levels of drug. Orange traffic cones, be afraid . . . and maybe pedestrians too.
So who wins this debate? As it turns out, the opponents agree on several key points. First of all, pot smoking is bad, and we cannot recommend the use of smoked cannabis in kids. Purified cannabinoids, on the other hand, are an intriguing prospect. We have isolated and studied the active compounds in marijuana, identified their biological receptors and endogenous ligands, and begun to accumulate limited efficacy and safety data for cannabinoids in the adult pain population. Little is currently known about the long term adverse effects of cannabinoids, and high-quality ethical research is badly needed before we can consider wide application in the pediatric pain population.
ASA Meeting Reviews
Pediatric Pain Poster Session
By Rita Agarwal, MD, FAAP
Children’s Hospital Colorado
Moderated by Drs. Jeffrey Galinkin and Mark Singleton
This was a well-attended and organized session reviewing some of the latest research in the field of pediatric pain medicine. The new HD poster screens were set up so that each poster was displayed on a separate screen and the audience could walk around review them at their leisure. After 20 minutes or so, each presenter came to the front of the room and using an even larger screen summarized their posters. The moderators made good use of the technology by zooming in on appropriate graphs, diagrams or paragraphs.
The first presentation was TAOK3: A Novel GWAS Locus Associated With Morphine Requirement and Postoperative Pain in Pediatric Day Surgery Scott D. Cook-Sather, MD et.al from the Department of Anesthesiology and Critical Care Medicine, Children's Hospital of Philadelphia and the Perelman School of Medicine at the University of Pennsylvania, Philadelphia, PA. The authors used Genome-Wide Association Studies (GWAS) to investigate Single Nucleotide Polymorphism associations with total morphine requirement in opioid-naïve children age 4 - 18 y undergoing day surgery tonsillectomy and adenoidectomy. These were children who had been previously extensively phenotyped. The authors chose children of European Caucasian ancestry to minimize heterogeneity. They were able to identify a novel SNP at the TAOK3 locus that correlated with increased morphine requirements.
Is Post-Thoracotomy Pain Being Managed Well in our Tertiary Referral Paediatric Hospital?
Fiona Desmond, MB,B.Ch et.al Dept of Anaesthesia and Critical Care Medicine, Our Lady’s Hospital for Sick Children, Dublin, Ireland, Dr. Desmond and her colleagues evaluated the use of extra-pleural and paravertebral catheters for post-operative thoracotomy children at her institution. They discovered that the catheters were not being used to their maximal potential and patients were often on both a local anesthesia infusion via the catheter and an intravenous infusion of opiate. Further nursing education might help improve analgesia and decrease the use of concurrent infusion
Assessment of the Withdrawal Assessment Tool (WAT-1) in Children with Congenital Heart Disease: A Retrospective Pilot Study Allison M. Fernandez, M.D.1, Constance L. Monitto, M.D.2. 1Anesthesia & Critical Care, All Children's Hospital, Saint Petersburg, FL, USA, 2Anesthesia and Critical Care Medicine, Johns Hopkins University, Baltimore, MD, USA. The Withdrawal Assessment Tool-version 1 (WAT-1) is currently the only validated tool for assessing opioid withdrawal in pediatric patients. It has never been tested in children who are recovering from congenital cardiac surgery. In this retrospective review the authors found that elevated WAT-1 scores frequently occurred, even in the absence of opioid weaning. They concluded that in patients with CHD the WAT-! Score was neither accurate nor specific for signs of opioid withdrawal.
Effect of Dexamethasone or Clonidine When Given as an Adjunct to Ropivacaine for Caudal Analgesia on Duration of Analgesia Compared to Placebo in Children Samia N. Khalil, M.D. et.al Anesthesiology, The University of Texas Medical School at Houston, Houston, TX, The authors investigated the effect of a single preservative free dose of dexamethasone of the duration of action a caudal block performed for out-patient surgery in children. They used ropivacaine 0.2% in addition to placebo, clonidine or 200ug of dexamethasone. Families were called to determine when they thought the child was in pain and required additional analgesia. It appeared that dexamethasone increased the time to first analgesia.
The Role of Epidural Analgesia in the Perioperative Pain Management of Pediatric Patients With Median Arcuate Ligament Syndrome Alina Lazar, MD et.al , University of Chicago, Chicago, IL, USA, University of Chicago, Chicago, IL, USA. Median Arcuate Ligament syndrome is a rare cause of chronic abdominal pain that can be relieved with laparoscopic release of the ligament. This retrospective chart review sought to determine the impact of epidural analgesia on post-operative outcome. Patients who had been on chronic analgesia were more likely to receive an epidural in the OR, than those who had been on no medications or non-opioid medication only. There was no difference overall in the length of admission and morphine equivalent use in either group, except for those patients who had had chronic opioid use. In that group epidural analgesia seemed to improve outcome.
Pharmacogenetics of Celecoxib in Children Post Adenotonsillectomy Kimmo Murto, MD, Christine Lamontagne, MD et.al. Children's Hospital of Eastern Ontario, Ottawa, ON, Canada. Human studies show a decrease clearance of celecoxib in patients with the CYP2C9 *3 allele. The authors of this fascinating study sought to determine the incidence of this allele in a population of healthy children undergoing T&A. There was a 7% incidence of the allele in this population, but no difference in pain scores in any of the groups. There were no adverse effects from the celecoxib.
Low Dose Ketamine Infusion Does Not Change Opioid Requirement After Pediatric Scoliosis Surgery. Sophie R. Pestieau, M.D et. al Division of Anesthesiology & Pain Medicine, The Sheikh Zayed Institute for Surgical Innovation, Children’s National Medical Center, Washington, DC. The perioperative use of low dose ketamine has been shown to decrease opioid consumption in a variety of surgical patients. Single dose ketamine has not been shown to be effective in patients undergoing posterior spinal fusions. The authors investigated the effect of a bolus plus a low dose infusion rate in the perioperative period in this patient population. Ketamine infusion continued for 72 hours post-operatively. There was no difference in opioid consumption or pain and sedation score, either at rest or with cough.
Single-Shot Caudal Block Versus Ultrasound-Guided Ilioinguinal/Iliohypogastric Nerve Block for Pediatric Orchidopexy. Yasuo Suzuki, MD et.al. Tokyo Metropolitan Children's Medical Center, Tokyo, Japan. Caudal analgesia has become a very common method for providing post-operative analgesia in patients undergoing orchiopexy. The authors compared the use of U/S guided ilioinguinal/iliohypogastric nerve block for unilateral orchiopexy repair with a stander caudal. All patients had blocks placed after induction of anesthesia and all patients received fentanyl at the beginning of anesthesia. The authors found that analgesia consumption and pain scores were similar in a both groups of patients.
LINKS:
Spine Surgery: An Update
By Cheryl K. Gooden, MD
Mount Sinai Medical Center, New York
This Sunday morning panel moderated by Mary McCann, MD (Boston Children’s Hospital) provided an overview of recent advances in the perioperative management of the pediatric patient undergoing spine surgery. The first speaker Deborah Rusy, MD (University of Wisconsin – Madison) presented “Intraoperative Neurophysiologic Monitoring for Spine Surgery.” She began by highlighting the past and current state of spine surgery as well as potential neurologic complications. Dr. Rusy provided a concise review of monitoring techniques. She concluded her presentation by describing factors that affect the various monitoring techniques.
Susan Goobie, MD (Boston Children’s Hospital) presented “Antifibrinolytic Use in Spine Surgery.” Dr. Goobie began by highlighting the antifibrinolytic agents that are currently available. Blood conservation strategies play an important role in the reduction in perioperative blood loss. However, much of the data on the efficacy of antifibrinolytics is based on studies in the adult population. Dr. Goobie directed the audience to an article (Anesthesiology 2011;114:862-71) in which she and other investigators examined the use of tranexamic acid in children undergoing craniosynostosis reconstruction surgery.
The results of their study demonstrate that tranexamic acid is effective in reducing perioperative blood loss and transfusion requirement. She concluded her discussion with the future direction of blood conservation in pediatrics might include nafamostat mesilate (NM), that has anticoagulation and anti-inflammatory properties.
The final speaker in this panel was Sabine Kost-Byerly, MD (Johns Hopkins Hospital) who presented “Spine Surgery: An Update – Pain Management.” She emphasized the use of multimodal pain and symptom management. Dr. Kost-Byerly discussed various intraoperative and postoperative treatment options that include acetaminophen, ketorolac, methadone, ketamine, gabapentin, clonidine and dexmedetomidine.
Pro vs. Con: Parental Presence in the Operating Room
Pro
By Elizabeth S. Yun, MD
University of Wisconsin School of Medicine
Madison, WI
For many families the induction of a general anesthesia is one of the most stressful times of the surgical experience. Over the years many studies have noted that when preoperative anxiety is left untreated, pediatric patients often suffered short and long term adverse consequences, such as postoperative agitation and regressive behaviors. While all studies agree that this problem must be addressed to ensure a positive experience for both patient and parents, much confusion exist regarding the most effective treatment. This review focuses on the use of parental presence as one important therapeutic intervention for this complex issue.
For many anesthesiologists, premedication with midazolam remains the most common treatment. Midazolam can be given orally and has a predictable onset time and a relatively short duration of action. Many studies show that this drug is a very effective treatment for anxiety, even when compared to parental presence. However, midazolam does have some issues. Even with commercial oral preparations, it has a less than pleasant taste, leading to poor patient compliance. Some patients may develop a paradoxical reaction to this drug as manifested by increased excitability. There is also been controversy regarding the role of preoperative midazolam in prolonging recovery and discharge of patients.
Because of these issues, newer drugs such as clonidine and dexmedetomidine are being used. While these drugs have less delirium and fewer paradoxical effects compared to midazolam, they have a slower onset of action. Clonidine can be given orally but dexmedetomidine can only be given intranasally. As with midazolam, patient noncompliance remains a problem. The child may not take the entire dose, and thus may not receive the benefit of the medication. Forcing a child to take a medication creates more anxiety for the family. Therefore, other interventions need to be considered.
One option is having a parent present with the child at the time of induction. However for many centers, allowing parental presence is not a simple option. Additional personnel need to be available to monitor parents and escort them from the operating room, adding a possible expense to the process. There is also the medical legal issue of having people misinterpreting treatment during a critical event. Furthermore, many studies have shown that midazolam is more effective than parental presence for treating a child’s anxiety. Moreover, a recent Cochrane review on nonpharmacologic treatment of preoperative anxiety concluded that there was no support in the literature for the effectiveness of parental presence compared to distraction techniques (7).
However the same Cochrane review noted the difficulties in forming a consensus from the individual studies. Different measures of anxiety and distress were used among all of the studies making comparisons across the studies difficult. The intervention could not be blinded to the providers since anxiety assessment was done by direct observation. Many studies included other interventions such as premedication and parental presence at the same time. Many studies also included parents’ self-reporting of their child’s and their own anxiety. Based on these findings, the evaluation of the effectiveness of parental presence has no clear answer at this time (7).
Despite these findings parents still want to have a voice in their child’s care. In response to this desire, family center care with parents as active participants now plays a significant role in many pediatric hospitals. An example is parental presence during pediatric resuscitation. A literature review by Dingeman and colleagues noted that parents want to be present at critical times in their child’s life. According to this review, parents did not interfere with the care of their child during critical events. Furthermore, parents who were present during resuscitation reported less anxiety, more knowledge of their child’s illness and treatment, and more acceptance of the outcome. The review did not find any support for increased medical legal issues.
Today, the AAP and the American Heart Association endorse giving parents the choice to stay with their child. These principles can be extended to the operating room (3). Chorney and Kain describe a family centered approach for the operating room. The preparation starts in the preoperative period with a multimodal intervention that provides information to both parent and child. In the intraoperative period, parents and clinicians would collaborate on a preoperative anxiety management plan, including parental presence in the operating room. Postoperatively, parents would be allowed in the recovery room with support from hospital personnel (1).
Other tools for managing preoperative anxiety include distraction with electronic devices and other tools. The Cochrane review noted that these therapies, whether devices or specially trained clowns were shown to have modest effect. Another approach proposed by Martin and colleagues is to help healthcare providers effectively communicate with children to reduce anxiety. They suggested that desirable behaviors include nonprocedural talk, developmentally appropriate procedural summary and avoiding apologizing, reassuring and empathizing statements. These strategies could be incorporated in the intraoperative phase of a family centered approach (7).
In light of these new findings, the role of the parent in the operating room needs to be redefined in the context of family center care. As described in an editorial by Lewis, this approach of engaging and educating the family may contribute to improved safety, reduced infection rate and better patient outcomes (5). Perhaps the best way to treat preoperative anxiety in a child is to utilize this model. By working in collaboration with parents, an effective anxiety management plan can be developed using premedication, distraction and effective communication behavior from both parents and healthcare providers.
While there might be some cost due to increased personnel for assisting the parents, the cost could be made up with less need for medications, less time spent in the operating room dealing with an anxious child or with prolonged recovery time because of emergence delirium or being too sedated. While more studies need to be done to measure effectiveness, these new strategies demonstrate ways the anesthesiologist can incorporate family centered care for parents and children in the operating room.
References
- Chorney JM and Kain ZN. Family Centered Pediatric Perioperative Care. Anesthesiology 2010; 112:751-755.
- Davison A and McKenzie I. Distress at Induction: prevention and consequences. Curr Opin Anesthesiol 2011; 24:301-306.
- Dingeman RS et al. Parental Presence During Complex Invasive Procedures and Cardiopulmonary Resuscitation: A Systematic Review of the Literature. Pediatrics 2007; 120: 842-854.
- Kain ZN, et.al. Family-centered Preparation for Surgery Improves Perioperative Outcomes for Children. Anesthesiology 2007; 106: 65-74.
- Lewis EH. A Culture Shift: Principles and Values of Patient and Family-centered Care: Changing the Patient and Provider Experience. Anesth Analg 2013; 116:1191-1192.
- Rosenbaum AN et.al Pro-Con Debate: The place of premdication in pediatric practice. Pediatr Anesth 2009; 19:817-828.
- Yip P et.al. Non-pharmacological interventions for assisting the induction of anaesthesia in children. Cochrane Database of Systemic Review 2009, Issue 3 Art. No. CD006447.
Con
By Douglas R. Thompson, MD
Department of Anesthesiology and Pain Medicine
Seattle Children’s Hospital
University of Washington
Seattle, WA
In academic medicine we often pride ourselves in adhering to ‘evidence based medicine.’ Interestingly, such aspirations seem to fall to the wayside when it comes to the question of allowing parental presence during induction of anesthesia (PPDI) in our pediatric patients.
In a nationwide survey in 1995 Kain et al.1 found that while the majority of adult patients received a sedating pre-medication, the majority of pediatric patients entered the operating room unmedicated and alone. A follow-up survey by Kain2 in 2002 revealed that 50% of respondents never allowed PPDI. Why would so many respondents be unwilling to allow parents to be present as their child was being induced for anesthesia?
Does the condition of a child at the time of induction really matter? Even if a child has a traumatic experience as they drift off to sleep, surely it is such a transient event that once the procedure is over the memory of induction will be rapidly forgotten. As reassuring as such a line of reasoning may be to an anesthesiologist whose patient has a tumultuous induction, evidence unfortunately is not supportive.
J Aono et al.3 showed that pre-school aged children exhibiting anxious behavior prior to induction of anesthesia had significantly higher levels of the stress hormones cortisol, epinephrine and norepinephrine. Also of significance to the perioperative management of pediatric patients, in 1996 Kain et al.4 showed that children who were very anxious on induction of anesthesia were at higher risk of negative behavioral problems later, including aggression, separation anxiety, eating disorders and temper tantrums.
In a separate study in 2004, Kain5 showed that children with more intense preoperative anxiety were more likely to show symptoms of emergence delirium in the PACU. Furthermore, Kain6 went on to show that preoperative anxiety in children correlated with significantly more pain during hospitalization and during their first three days at home post hospitalization.
It is revealing that the preoperative experience can have such a profound and lasting effect on a child’s incidence of emergence delirium, postoperative behavior and postoperative pain scores. Given the preponderance of evidence in support of the importance of alleviating a child’s anxiety prior to anesthetizing them, it would seem obvious that as anesthesiologists entrusted with the care of these developing individuals we would do all we can to allay their fears and provide as stress-free an experience as possible. So the question arises, is allowing a parent to be present during induction of any real benefit to our patients? How should ‘evidence based medicine’ guide our actions? To answer these questions we turn to scientific studies on the topic.
In 2009 Chundamala et al.7 conducted a review of fourteen studies examining the effect of parental presence during the induction of anesthesia. Eleven of the fourteen studies looked at the impact on the child’s anxiety. The vast majority of these studies showed NO difference in patient anxiety regardless of whether or not parents were present. In fact, there were only two studies which demonstrated that having a parent attend the induction was of any benefit to the child. Furthermore, in a Cochrane review of seventeen studies conducted in 2010 by Yip et al.8, the authors concluded, “This review shows that the presence of parents during induction of general anaesthesia does not reduce their child’s anxiety.”
In a study not covered in the Cochrane review, Kazak et al.9 again showed that parental presence alone was not efficacious in reducing separation anxiety in the preoperative setting. Vagnoli et al.10 showed that having a clown present during induction was more effective in anxiolysis than having a parent present. It should also be pointed out that in some cases, having a parent present can actually make matters worse. In a study by Bevan et al.11, children of ‘anxious’ parents were significantly more distraught with parental presence than without.
If having a parent attend the induction of anesthesia is so ineffective in allaying patient anxiety, what are some examples of successful interventions?
In 1998 Kain et al.12 examined anxiety scores in children randomized to either parental presence or midazolam premedication. Not surprisingly, children in the midazolam group showed significantly less anxiety at separation, entry to OR and introduction of the mask. As an aside, parents in the midazolam group were also significantly less anxious.
In 1999 Kain13 showed that the lower preoperative anxiety scores that resulted from midazolam premedication also translated into significantly lower incidence of negative behavioral problems postoperatively. This difference persisted for up to two weeks. Similarly, Kazak et al.9 also showed midazolam premedication to be an effective preoperative anxiolytic for children.
In addition to pharmacologic methods, other distraction techniques have been shown to be effective as well. Patel et al.14 showed that children playing a video game while their parent was present during induction of anesthesia had a significantly lower increase in anxiety scores on induction than children in the parental presence only arm of the study. Hypnosis has been shown to be effective in reducing negative postoperative behavior compared to midazolam premedication; hypnosis also demonstrated a trend towards reducing anxiety during induction.15 Kain et al.16 showed that a low sensory stimulation environment in the operating room contributed to a significantly less anxious patient on entrance to the operating room and induction compared with the control group. Finally, children of parents who underwent an anxiety-reducing acupuncture treatment were significantly less anxious during entrance to the OR and introduction of the anesthesia mask.17
It may be difficult to believe or to convince parents of the facts, but evidence has repeatedly shown that simply having a parent present for induction is of little or no benefit to the child. In addition to offering no advantage to the child, allowing a parent to be present for induction can present significant additional risk.
For example, reports have described parents removing their child from the operating room stretcher and monitors during induction.18 As with other aspects in medicine, we must ask ourselves if the evidence supports benefits and risks of our management. In the case of parental presence during induction, the preponderance of evidence suggests the answer is no.
References
- Kain ZN, Mayes LC, Bell C, et al. Premedication in the United States: a status report. Anesth Analg 1997;84:427–32.
- Kain et al. Parental Presence and Sedatives: A follow-up study Anesth Analg 2004;98:1252–9
- J Aono et al. Differences in hormonal responses to preoperative emotional stress between preschool and school children Acta Anaesthesiol Scand 1997;41:229-231.
- Z Kain et al. Preoperative Anxiety in Children Predictors and Outcomes Arch Pediatr Adolesc Med 1996; 150: 1238-1245.
- Z Kain et al. Preoperative Anxiety and Emergence Delirium and Postoperative Maladaptive Behaviors Anesth Analg 2004; 99: 1648-54.
- Z Kain et al. Preoperative Anxiety, Postoperative Pain, and Behavioral Recovery in Young Children Undergoing Surgery Pediatrics 2006; 118: 651-658.
- Chundamala et al. An evidence-based review of parental presence during anesthesia induction and parent/child anxiety Can J Anesth 2009; 56: 57-70.
- Yip P, Middleton P, Cyna AM, Carlyle AV. Non-pharmacological interventions for assisting the induction of anaesthesia in children. Cochrane Database of Systematic Reviews 2009, Issue 3. Art. No.: CD006447. DOI: 10.1002/14651858.CD006447.pub2.
- Kazak et al. Premedication with oral midazolam with or without parental presence Eur J Anaesthesiol 2010;27:347–352 .
- Vagnoli L, Caprilli S, Robiglio A, Messeri A. Clown doctors as a treatment for preoperative anxiety in children: a randomized,prospective study. Pediatrics 2005;116:563–7.
- Bevan JC, Johnston C, Haig MJ, Tousignant G, Lucy S, Kirnon V,et al. Preoperative parental anxiety predicts behavioural and emotional responses to induction of anaesthesia in children. Canadian Journal of Anaesthesia 1990;37:177–82.
- Z Kain et al. Parental Presence During Induction of Anesthesia versus Sedative Premedication Anesthesiology 1998; 89:1147-56.
- Z Kain et al. Postoperative Behavioral Outcomes In Children Effects of Sedative Premedication Anesthesiology 1999; 90: 758-65
- Patel A, Schieble T, Davidson M, Tran MC, Schoenberg C, Delphin E, et al. Distraction with a hand-held video game reduces pediatric preoperative anxiety. Pediatric Anesthesia 2006;16: 1019–26.
- Calipel S, Lucas-Polomeni MM, Wodey E, Ecoffey C. Premedication in children: hypnosis versus midazolam. Pediatric Anesthesia 2005;15:275–81.
- Kain ZN, Wang SM, Mayes LC, Krivutza DM, Teague BA. Sensory stimuli and anxiety in children undergoing surgery: a randomized, controlled trial. Anesthesia and Analgesia 2001;92:897–903.
- Wang SM, Maranets I, Weinberg ME, Caldwell-Andrews AA, Kain ZN. Parental auricular acupuncture as an adjunct for parental presence during induction of anesthesia. Anesthesiology 2004;100:1399–404.
- Johnson YJ, Nickerson M, Quezado ZMN. An Unforeseen Peril of Parental Presence During Induction of Anesthesia. Anesth Analg December 2012 115:1371-1372.
![]()
Pediatric Dental Emergencies Associated with Endotracheal Intubation
By Rebeca Urquiola, DDS; Hassan Oueis, DDS
Department of Pediatric Dentistry
University of Detroit-Mercy
Detroit, MI
Zulfiqar Ahmed, MD
Anesthesia Associates of Ann Arbor
Dearborn, MI
Dental injury is a common complication during general anesthesia. Only a few studies have addressed the extent and nature of the problem in children. In order to reduce dental emergencies during intubation in the pediatric dental patient, prophylactic measures should be taken before endotracheal intubation
Preoperative Prophylactic Measures
In planning for general anesthesia, the patient may need to have a dental examination and should obtain a clearance from his/her dentist if appropriate. The dentist should address dental disease, if present, and potential risk that can be encountered during airway manipulation of airway for general anesthesia (newly erupted teeth, mobile teeth, prosthetic appliances, orthodontic appliances, periodontal disease, and active dental caries). In order to facilitate the anesthesia management, the dentist should provide emergent treatment (e.g. removal of mobile teeth, badly decayed teeth or removal of fixed orthodontic appliances) if time permits. All removable prosthetic and/or orthodontic appliances should be taken out of the mouth of the patient at the day of surgery. The anesthesia team should inform parents about the potential of trauma to natural teeth during anesthesia. Consent should be also obtained from parents according to institutional protocol.
Traumatic injuries and their management
Enamel fractures. For permanent teeth:
- Locate the fragment(s).
- Place fragment in Hank’s solution, milk, or patient’s own saliva.
- Contact dentist for evaluation and schedule treatment once patient is medically stable.
For primary teeth, although no treatment is indicated, contact dentist for thorough evaluation once the patient is medically stable.
Enamel-dentin fractures. For permanent teeth:
- Locate fragment(s).
- Place fragment in Hank’s solution, milk, or patient’s own saliva.
- Contact dentist for evaluation and schedule treatment once patient is medically stable.
For primary teeth, contact dentist for thorough evaluation and treatment once the patient is stable.
Enamel-dentin fracture with pulp exposure. For permanent teeth:
- Locate fragment(s).
- Place fragment in Hank’s solution, milk or patient’s own saliva.
- If bleeding form pulp tissue is present, apply pressure with Hank’s moistened gauze until bleeding stops.
- Contact dentist for evaluation and schedule treatment once the patient is medically stable.
For primary teeth, if bleeding is present, apply pressure with Hank’s moistened gauze until bleeding stops. Contact dentist for evaluation and treatment once the patient is medically stable. In general the treatment involves extraction of the affected tooth.
Crown-root fracture with pulp exposure. For permanent teeth:
- Locate crown-root fragment (s)
- Place in Hank’s solution, milk or patient’s own saliva.
- Stop bleeding from pulp by applying continuous pressure for few minutes with Hank’s moistened gauze. The process may be repeated until bleeding stops.
- Contact dentist for evaluation and to schedule emergency dental visit as soon as patient is medically stable.
For primary teeth, remove the coronal portion of the tooth, stop bleeding with continuous pressure for few minutes. Contact dentist for evaluation and extraction of the remaining portion of the tooth once the patient is medically stable.
Tooth avulsion (out of the socket). For permanent teeth:
- Time is critical for this kind of dental injury
- Locate tooth.
- If the anesthesia team concludes that replanting the avulsed tooth during or immediately after surgery creates a high risk for aspiration, do not replant. Place the avulsed tooth in Hank’s solution, milk or patient’s own saliva.
- Have patient seen by a dentist as soon as possible. Be aware that if the avulsed tooth cannot be replanted within 60 minutes after avulsion the prognosis of the tooth to survive is very poor.
- If replanting, grasp the tooth by the coronal portion (whiter portion of the tooth) with a Hank’s moistened gauze. Gently, rinse the tooth with Hank’s solution and reposition it into the socket. Apply digital pressure, and if bleeding is present keep providing digital pressure until it stops. Do not touch the radicular portion (root) since you may damage fibers important for the healing process.
- Once active bleeding stops, contact dentist for evaluation and pertinent treatment once patient is medically stable.
For primary teeth: do not re-implant primary teeth, stop bleeding with continuous pressure for few minute. Contact dentist for evaluation once the patient is stable.
Tooth luxation. The change of tooth position due to trauma from an instrument with or without fracture. For permanent teeth:
- Using a Hank’s moistened gauze, grasp tooth by the crown and reposition it into its original position.
- Contact dentist for evaluation and to schedule a proper treatment once the patient is medically stable.
For primary teeth: using a Hank’s moistened gauze, grasp tooth by the crown and reposition it into its original position for minor laxation. Assess tooth mobility and if mobility of tooth is at high risk of aspiration, remove tooth and control bleeding with soft finger pressure. Contact dentist for evaluation once the patient is stable.

![]()
PedsPassport: Your global meeting itinerary
By Helen V. Lauro, MD, MPH, MSEd, FAAP
NOTE: Purchase of travel insurance with air evacuation coverage
is highly recommended to meeting attendees and their families
2014
February 14-16: Anaheim, California, United States
52nd Clinical Conference in Pediatric Anesthesiology
Tel: (323) 261-2262, Fax: (323) 361-1001
Information: Eenar Lee, Pediatric Anesthesiology Foundation and Children's Hospital Los Angeles, 4650
Sunset Blvd, Mail Stop:MS #3, Los Angeles, California, 90027
Website: http://pediatric-anesthesiology-foundation.org/?page_id=6
E-Mail: eelee@chla.usc.edu
February 19-23: Lake Buena Vista, Florida, USA
17th Annual Update on Pediatric and Congenital Cardiovascular Disease
Tel: (215) 590-5263, Fax: (215) 590-4342
Information: Ms. Micah Holliday, Continuing Medical Education Department, The Children's Hospital of
Philadelphia, 34th Street and Civic Center Boulevard, Philadelphia, PA 19104-4399
Website: http://www.chop.edu/cardiology2014
February 21-23: Panjim, Goa, India
6th National Conference on Paediatric Anaesthesia (Jointly organized by Indian Association of Paediatric Anaesthesiologists & Goa Medical College)
Tel: (91) 2224126068/02224126202
Information: Dr. Pradnya Sawant, Department of Anaesthesia, Library at B. J. Wadia Hospital for Children,
Acharya Donde Marg, Parel. Mumbai - 400 012.
Website: http://www.iapa-india.org
Email: drpradnyas@hotmail.com, paedsanaesthesia2014@gmail.com
March 6: Fort Lauderdale, Florida, USA
Congenital Cardiac Anesthesia Society 2014 Meeting
Tel: (804) 282-9780, Fax (804) 282-0900
Information: Congenital Cardiac Anesthesia Society, 2209 Dickens Road, Richmond, VA 23230-2005
Website: http://www.ccasociety.org
Email: ccas@societyhq.com
March 6: Fort Lauderdale, Florida, USA
Society for Pediatric Pain Medicine 1st Annual Meeting
Tel: (804) 282-9780, Fax (804) 282-0900
Information: Society for Pediatric Pain Medicine, 2209 Dickens Road, Richmond, VA 23230-2005
Website: http://www.pedspainmedicine.org
Email: sppm@societyhq.com
March 7-9: Fort Lauderdale, Florida, USA
Society for Pediatric Anesthesia (SPA)/American Association of Pediatrics (AAP) Pediatric Anesthesiology 2014 Meeting
Tel: (804) 282-9780, Fax (804) 282-0900
Information: Society for Pediatric Anesthesia, 2209 Dickens Road, Richmond, VA 23230-2005
Website: http://www.pedsanesthesia.org
Email: spa@societyhq.com
April 23-25: Vienna, Austria
6th International Pediatric Simulation Symposia and Workshops
Tel: + 32 2 7402254
Information: International Pediatric Simulation Society, Avenue de Tervueren, 300 B-1150 Brussels,
Belgium
Website: www.ipedsim.com
Email: info@ipedsim.com
May 2-4: Boston, Massachusetts, USA
Principles of Pediatric Anesthesiology and Critical Care
Tel: (617) 384 8600; Fax: (617) 730-0894
Information: Mary Duross, Department of Anesthesiology, Perioperative and Pain Medicine, Boston
Children's Hospital, 300 Longwood Ave, Boston, Massachusetts, 02115
Website: http://cme.hms.harvard.edu/index.asp?SECTION=CLASSES&ID=00342645&SO=N#geninfo
E-Mail: hms-cme@hms.harvard.edu
May 2-4: Southlake, Texas, USA
Pediatric Anesthesia Conference - Improving the quality of care: Evidence-based plans for common concerns
Tel: (682) 885-3841, Fax: (982) 885-6140
Information: Ms. Breanna Anderson, Department of Education, Cook Children's Hospital, 801 Seventh
Avenue, Fort Worth, Texas, 76104-2796
Website: https://secure.cookchildrens.org/Education/CourseFiles/2014%20PAC%20Agenda_FINAL.pdf
E-Mail: breanna.Anderson@cookchildrens.org
May 4-7: Istanbul, Turkey
7th World Congress on Pediatric Intensive and Critical Care (PICC 2014)
Tel: +41 22 9080488., Fax: +41 22 9069140
Information: Kenes International Ltd, 1-3 Rue de Chantepoulet, P.O. Box 1726, CH-1211, Geneva 1,
Switzerland
Website: http://www.kenes.com
Email: info@kenes.com
May 8-11: Istanbul, Turkey
12th Asian Society of Paediatric Anaesthesiologist Congress
Information: ASPA Secretariat, Department of Paediatric Anaesthesia, KK Women’s and Children’s
Hospital, 100 Bukit Timah Road, Singapore 229899
Website: http://aspaturkey2014.org/
Email: serpozgen@tnn.net
May 15-16: Leeds, United Kingdom
Association of Paediatric Anaesthetists of Great Britain and Ireland Meeting
Tel: +44 (0) 20 7631 8887, Fax: +44 (0) 20 76314352
Information: APA Administration Office, AAGBI, 21 Portland Place, London, W1B 1YP, United Kingdom
Website: http://www.apagbi2014.co.uk
Email: apaevents@aagbi.org
May 19-21: Charleston, South Carolina, USA
Society for Pediatric Sedation® Conference 2014
Great Expectations: Forging A Culture of Safety & Quality in Sedation Practice
Tel: (804) 565-6354, Fax: (804) 282-0090
Information: Society for Pediatric Sedation®, 2209 Dickens Rd., Richmond, VA 23230-2005
Website: http://www.pedsedation.org
Email: sps@societyhq.com
May 30-June 1: Dallas, Texas, USA
Intensive Review of Pediatric Anesthesia
Tel: (804) 282-9780, Fax: (804) 282-0090
Information: Society for Pediatric Anesthesia, 2209 Dickens Road, Richmond, VA 23230-2005
Website: http://www.pedsanesthesia.org
Email: spa@societyhq.com
June 12-15: Key West, Florida, USA
8th Annual Pediatric Anesthesia Review
Tel: (800) 222-6927
Information: Northwest American Seminars, P.O. Box 2797, Pasco, WA 99302
Website: http://www.nwas.com
Email: info@nwas.com
September 13: Dallas, Texas, USA
Dr. Jensen Anesthesiology Board PREP Pediatric Board Review Course
Tel: (800) 321-7737 or (319) 337-3700, Fax: (319) 341-9818
Information: Niels F. Jensen MD, Anesthesiology Board PREP, 235 Lexington Avenue, Iowa City, Iowa
52246
Website: http://www.anesthesiologyboards.com
Email: njensen@anesthesiologyboards.com
September 18-20: Prague, Czech Republic
Annual Congress of the European Society for Paediatric Anaesthesiology: Prague 2014
Tel: +420 284 001 444
Information: Congress Secretariat, GUARANT International spol. sr.o, Na Pankraci 17, 140 21 Prague 4,
Czech Republic
Website: http://www.euroespa.org, http://www.guarant.cz
Email: secretary@euroespa.org, espa2014@guarant.cz
September 26-28: Montreal, Quebec, Canada
Joint Canadian Pediatric Anesthesia Society (CPAS) and Association of Paediatric Anaesthetists of
Great Britain and Ireland (APAGBI) meeting 2014
Tel: (416) 480-0602, Fax: (416) 480-0320
Information: Canadian Pediatric Anesthesia Society, c/o Canadian Anesthesiologists’ Society, 1 Eglinton Ave
East, Suite 208, Toronto, ON M4P 3A1
Website: http://www.pediatricanesthesia.ca/about/contact-us/
October 1-3: Newcastle, United Kingdom
PICS- 28th Annual Paediatric Intensive Care Society Conference
Tel: +44 (0) 207 383 8030
Information: Kenes International Ltd., One Euston Square, 40 Melton Street, London NW12FD
Website: http://www.kenes.com
Email: pics@kenes.com
October 10: New Orleans, Louisiana, USA
Society for Pediatric Anesthesia 28th Annual Meeting
Tel: (804) 282-9780, Fax (804) 282-0900
Information: Society for Pediatric Anesthesia, 2209 Dickens Road, Richmond, VA 23230-2005
Website: http://www.pedsanesthesia.org
Email: spa@societyhq.com
October 16-19: Hobart, Tasmania
Society for Paediatric Anaesthesia in New Zealand and Australia (SPANZA) 2014 Gems of Wisdom
Tel: + 61 2 4973 6573, Fax: + 61 2 4973 6609
Information: Meeting Secretariat, P. O. Box 180, Morisset, NSW 2264, Australia
Website: http://www.spanza.org.au
Email: spanzaconf@willorganise.com.au
October 17-21: Barcelona, Spain
25th Annual Congress of European Society of Paediatric and Neonatal Intensive Care (ESPNIC) in conjunction with the 5th Congress of the European Academy of Paediatric Societies (EAPS)
Tel: +41 22 9080488., Fax: +41 22 9069140
Information: Kenes International Ltd, 1-3 Rue de Chantepoulet, P.O. Box 1726, CH-1211, Geneva 1,
Switzerland
Website: http://www.kenes.com
Email: paediatrics@kenes.com
2015
March 12: Phoenix, Arizona, USA
Congenital Cardiac Anesthesia Society 2015 meeting
Tel: (804) 282-9780, Fax (804) 282-0900
Information: Congenital Cardiac Anesthesia Society, 2209 Dickens Road, Richmond, VA 23230-2005
Website: http://www.ccasociety.org
Email: ccas@societyhq.com
March 12: Phoenix, Arizona, USA
Society for Pediatric Pain Medicine 2nd Annual Meeting
Tel: (804) 282-9780, Fax (804) 282-0900
Information: Society for Pediatric Pain Medicine, 2209 Dickens Road, Richmond, VA 23230-2005
Website: http://www.pedspainmedicine.org
Email: sppm@societyhq.com
March 13-15: Phoenix, Arizona, USA
Society for Pediatric Anesthesia (SPA)/American Association of Pediatrics (AAP) Pediatric Anesthesiology 2015 Meeting
Tel: (804) 282-9780, Fax (804) 282-0900
Information: Society for Pediatric Anesthesia, 2209 Dickens Road, Richmond, VA 23230-2005
Website: http://www.pedsanesthesia.org
Email: spa@societyhq.com
May 31-June 4: Seattle, Washington, USA
10th International Symposium on Pediatric Pain 2015
Information: Ms. Lisa M. Peters, MN, RN, ISPP 2015 Organizing Committee Chair, Department of
Anesthesiology and Pain Medicine, Seattle Children's Hospital, 4800 Sand Point Way NE, Seattle,
Washington, 98105
Website: http://childpain.org
Email: ispp2015@seattlechildrens.org
September 23-25: Birmingham, United Kingdom
PICS- 29th Annual Paediatric Intensive Care Society Conference
Tel: +44 (0) 207 383 8030
Information: Kenes International Ltd., One Euston Square, 40 Melton Street, London NW12FD
Website: http://www.kenes.com
Email: pics@kenes.com
Footnote:
Please forward all information concerning congresses relevant to
Pediatric Anesthesia to:
Helen V. Lauro, MD, MPH, MSEd, FAAP, SUNY Downstate Medical Center University Hospital of Brooklyn at Long Island College Hospital, Department of Anesthesiology, 339 Hicks Street, Brooklyn, New York 11201.
![]()