
NM-313
Chronic Chest Pain Following Pectus Excavatum Repair
Sangari T, Kumar S, Islam S, Dooley C, Desmond M
University of Florida, Gainesville, FL, United states
Introduction: This case report illustrates the efficacy of radiofrequency ablations (RFA) for long-term pain relief of intercostal neuralgia due to intra-thoracic Nuss bar.
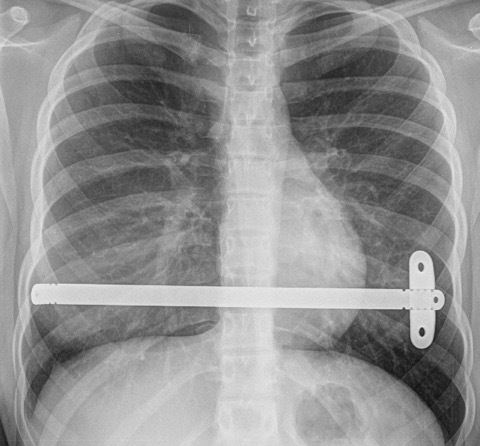
Case Report: 14-year-old, 55kg female presented to pain clinic with progressively worsening chest pain since her laparoscopic Nuss procedure for pectus excavatum. She was pain free for first two weeks’ post-surgery but started with bilateral costochondral sharp stabbing pain subsequently. Over six months her pain worsened from sharp to include burning sensation in the anterior chest wall. She rated pain 9/10 lifting objects and 5/10 at rest. This pain led to significant stress in her everyday life, affecting her sleep and school activities. Prior to presentation she was on ibuprofen and neurontin for 3 months with minimal relief. On examination pectus excavatum appeared corrected with well healed surgical scars. She was tender on palpation bilaterally at costochondral margins from T6 to T10. Chest X-ray illustrated NB in correct position (Fig1). Diagnosis of chronic bilateral T6-T10 intercostal neuralgia was established with fluoroscopic guided intercostal nerve blocks.
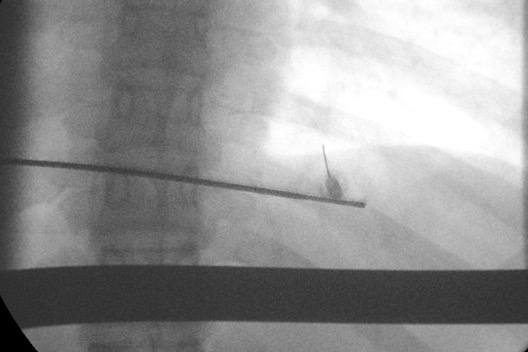
Procedure: Patient was placed in prone position with fluoroscopy guidance costal margins on right side from T6 to T10 level were identified. 2 ml of 1% lidocaine was injected for local infiltration. Following this, a 50mm, 22 gauge, curved RFA needle with a 5mm active tip was walked off the inferior coastal margin and guided to the target point at the intercostal groove (Fig 2). Motor stimulation at 2 Hz revealed no evidence of distal muscle contraction and sensory testing demonstrated radiating "tingling" into the painful area at each level.  Prior to lesioning, 0.5 mL of 2% lidocaine was injected and fluoroscopic image was obtained to confirm the position of needle. Two 90 seconds lesioning cycle at 80°C at each level on ipsilateral side were adminstered. Post procedure patient reported resolution of chest pain on the side of the ablation. Subsequently in two weeks’ patient received RFA on the left side, following which she reported complete resolution of her chest pain symptoms.
Discussion: This case demonstrates that conventional thermal RFA of the intercostal nerves is a viable and safe treatment for intercostal neuralgia secondary Nuss bar placement. This technique can be used to treat other pain conditions involving intercostal nerve, such as slip rib syndrome, post thoracotomy or blunt trauma pain in pediatrics.
Reference: Ladenhauf etal. Successful Treatment of Persistent Pain After Pectus Excavatum Repair Using Paravertebral Nerve Radiofrequency Thermoablation A&A Case Reports. 2017;8:18–20
-
 NM-313 Image 2
NM-313 Image 2 -
 NM-313 Image 1
NM-313 Image 1
Top










