
GA4-86
Occipital Nerve Blocks for Relief of Headaches in Patients with Ventriculoperitoneal Shunts
Jensen B, Kim E, Cucchiaro G
Children's Hospital Los Angeles, Los Angeles, CA, USA
Introduction- More than 3300 pediatric ventriculoperitoneal (VP) shunts are placed in the US annually.2 The most common reason for surgical revision is malfunction, with one study quoting 41% of all shunting procedures. Shunt malfunction commonly manifests as acute or chronic headache.3 Patients with VP shunts who present to the emergency room with headaches may often undergo evaluation for shunt revision. In this review, we looked at a series of patients with VP shunts and chronic recurrent headaches which resolved after occipital nerve blocks.
Materials and Methods- We reviewed the medical records of patients with a VP shunt who were seen by a pain specialist for occipital headaches. In addition to demographic data, primary diagnosis, VP shunt insertion and revision dates were recorded. Medications, placement of occipital nerve blocks, and follow-up including emergency room visits for headaches were also noted.
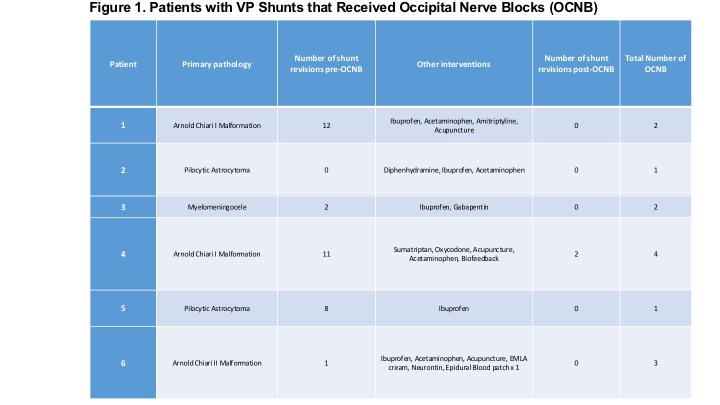
Results- Six patients with VPS received occipital nerve blocks for occipital headaches from 2011 to 2017. The majority of patients were female (83%) and age ranged from 15-20 years-old. Primary diagnosis included Arnold Chiari Malformation, Pilocytic Astrocytoma, and Myelomeningocele. 83% of patients had a history of at least one VP shunt revision. Occipital nerve blocks were performed via landmarks using Bupivacaine 0.25% and careful avoidance of VP shunt tubing.
All patients were noted to have improved headaches following the block. There were no complications reported. Four patients (66%) received repeat occipital nerve blocks with good relief. Four patients had subsequent emergency room visits for headaches. Of these, only one patient was found to have a shunt malfunction and the VP shunt was revised.
Discussion- Headaches in the setting of VP shunts can be difficult to diagnose and manage. Although shunt malfunction must be ruled out, a detailed physical examination is necessary and can help prevent unnecessary tests and operations. The shunt tubing or the valve itself may cross over the path of the greater or lesser occipital nerve resulting in headaches due to mechanical irritation of the occipital nerve.1 Persistent occipital headaches with tenderness and radiation in the path of the greater and lesser occipital nerves can be indicative of occipital neuralgia. Occipital nerve blocks can help as both diagnostic and therapeutic interventions in these patients.
References
1. Adult Hydrocephalus. Cambridge University Press, 2014.
2. Simon, Tamara D., et al. “Hospital Care for Children with Hydrocephalus in the United States: Utilization, Charges, Comorbidities, and Deaths.â€Â Journal of Neurosurgery: Pediatrics, vol. 1, no. 2, 2008, pp. 131–137., doi:10.3171/ped/2008/1/2/131.
3. Stone, Jonathan J., et al. “Revision Rate of Pediatric Ventriculoperitoneal Shunts after 15 Years.â€Â Journal of Neurosurgery: Pediatrics, vol. 11, no. 1, 2013, pp. 15–19., doi:10.3171/2012.9.peds1298.
-
 GA4-86 Image 1
GA4-86 Image 1
Top










