
CR2-184
Erector Spinae Plane Block for Chest Wall Deformity Surgery
Cheng T, Holland E, Bosenberg A
Seattle Children's Hospital, Seattle, WA, USA
BACKGROUND
Surgical correction of pectus excavatum and carinatum is associated with significant postoperative pain, which historically has been controlled with epidural analgesia. However, questions about the risk of thoracic epidurals in this patient population have been raised and many institutions have turned to alternatives for postoperative pain control.
The erector spinae plane (ESP) block is an ultrasound-guided technique involving injection of local anesthetic in a fascial plane deep to the erector spinae muscle. It is technically easier to perform than a paravertebral block and does not violate the neuraxial space, while potentially spreading craniocaudally in the paravertebral space, making it a promising option for postoperative pain control. Here we describe a series of 10 cases utilizing ESP blocks for chest wall deformity repair.
METHODS
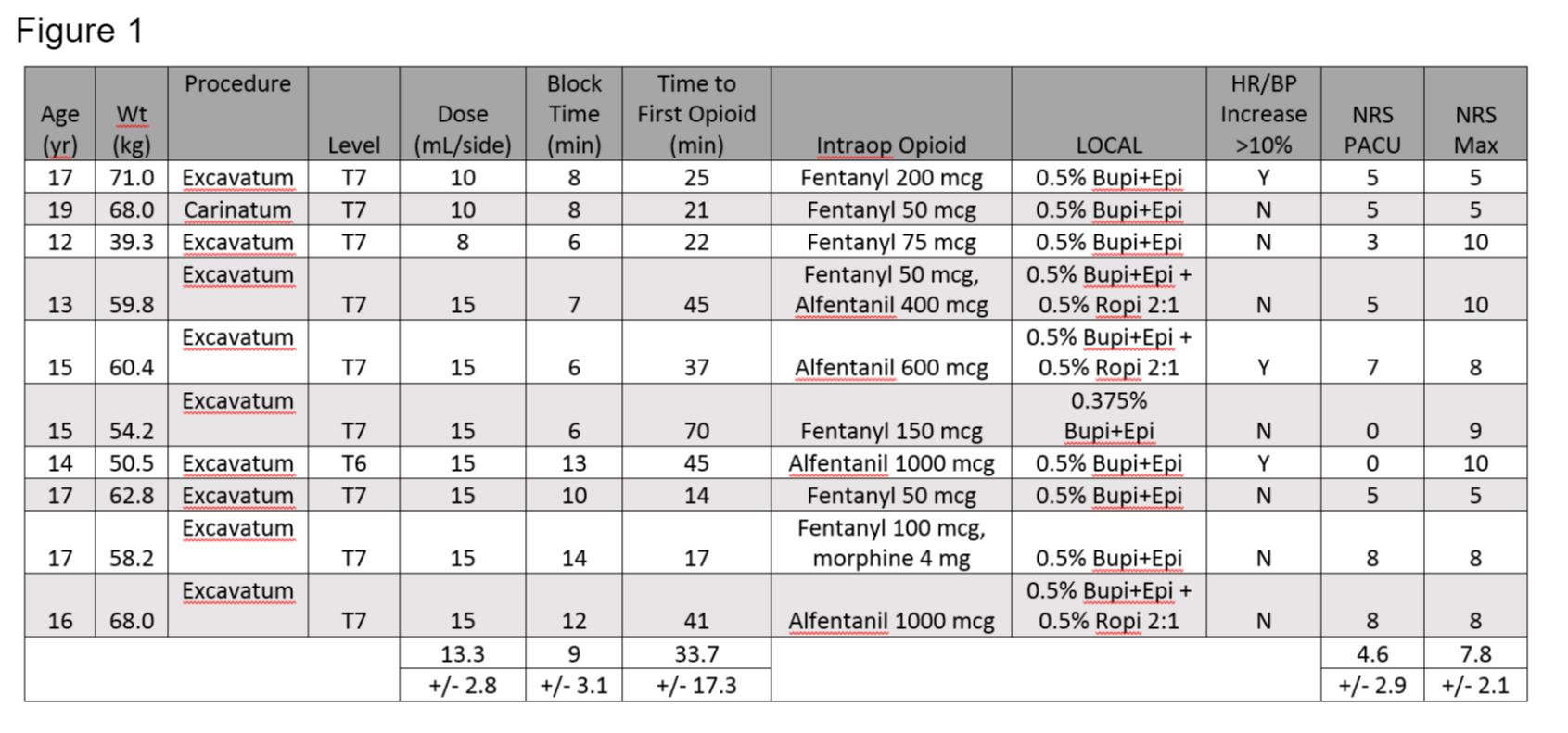
We identified 10 pediatric patients who received bilateral ESP block for chest wall deformity correction between June and October 2017 at a quaternary children's hospital. A retrospective chart review using the Pediatric Regional Anesthesia Network (PRAN) database was performed and data regarding block details, hemodynamic response to incision, opioid consumption, and postoperative pain scores were collected. All blocks were performed or supervised by a single anesthesiologist.
RESULTS
Average block time was 9 +/- 3.1 min, local anesthetic volume was 0.14 to 0.29 mL/kg per side and intraoperative fentanyl use was 1.2 mcg/kg (Figure 1). Only one patient received morphine. 3 of 10 patients had an increase in heart rate and blood pressure >10% with incision. Postoperatively, all patients were managed with continuous wound infiltration and patient-controlled opioid analgesics.
DISCUSSION
Single-shot ESP block is simple and quick to perform. Minimal hemodynamic response to incision and low intraoperative opioid consumption suggest that it is effective for pectus surgery. Patients had moderate-to-high postoperative pain scores and significant opioid requirement, suggesting that a single-shot block is inadequate for postoperative analgesia. As our current practice is to use continuous wound infiltration of local anesthetic, we have not yet evaluated continuous ESP catheters.
CONCLUSION
ESP block is a simple regional technique that can provide intraoperative analgesia for chest wall deformity correction. Further research is needed to evaluate its efficacy for postoperative pain control compared to the use of continuous wound infiltration
1. Kelly RE, et al. Twenty one years of experience with minimally invasive repair of pectus excavatum by the Nuss procedure in 1215 patients. Annals Surg 2010 Dec; 252 (6): 1072-81
2. Davies RG, et al. A comparison of the analgesic efficacy and side
effects of paravertebral vs. epidural blockade for thoracotomy — a systematic review and meta-analysis of randomized trials. Br J Anaesth 2006;96:418-26
-
 CR2-184 Image 1
CR2-184 Image 1
Top










