
NM-277
Methadone Loading for Minimally Invasive Repair of Pectus Excavatum
1Swathirajan, , 2Reece-Stremtan S, 2Cohen I
1Children's National Medical Center, Washington, DC, USA; 2CNMC, Washington, DC, USA
INTRODUCTION: Minimally Invasive Repair of Pectus Excavatum (MIRPE) is associated with significant postsurgical pain - traditionally managed at our institution with epidural analgesia. Secondary to anecdotal reports of spinal cord injuries with this technique, patient controlled analgesia with a continuous infusion (PCA-C) became our less-than-satisfactory treatment of choice. Based on previous reports, two faculty members piloted the use of an intraoperative methadone loading dose of 0.2mg/kg. We hypothesized that methadone’s long half-life and dual receptor action would result in lower pain scores and reduced PCA use.
METHODS: As a quality improvement project, a retrospective review of adolescents undergoing MIRPE was performed. Data collected included: daily maximum pain scores, total PCA demand doses received, and pro re nata (PRN) doses of diazepam, ondansetron and opioid. Data were compared between patients who had and had not received methadone intraoperatively. Descriptive, parametric, and non-parametric statistics were used to analyze our findings.
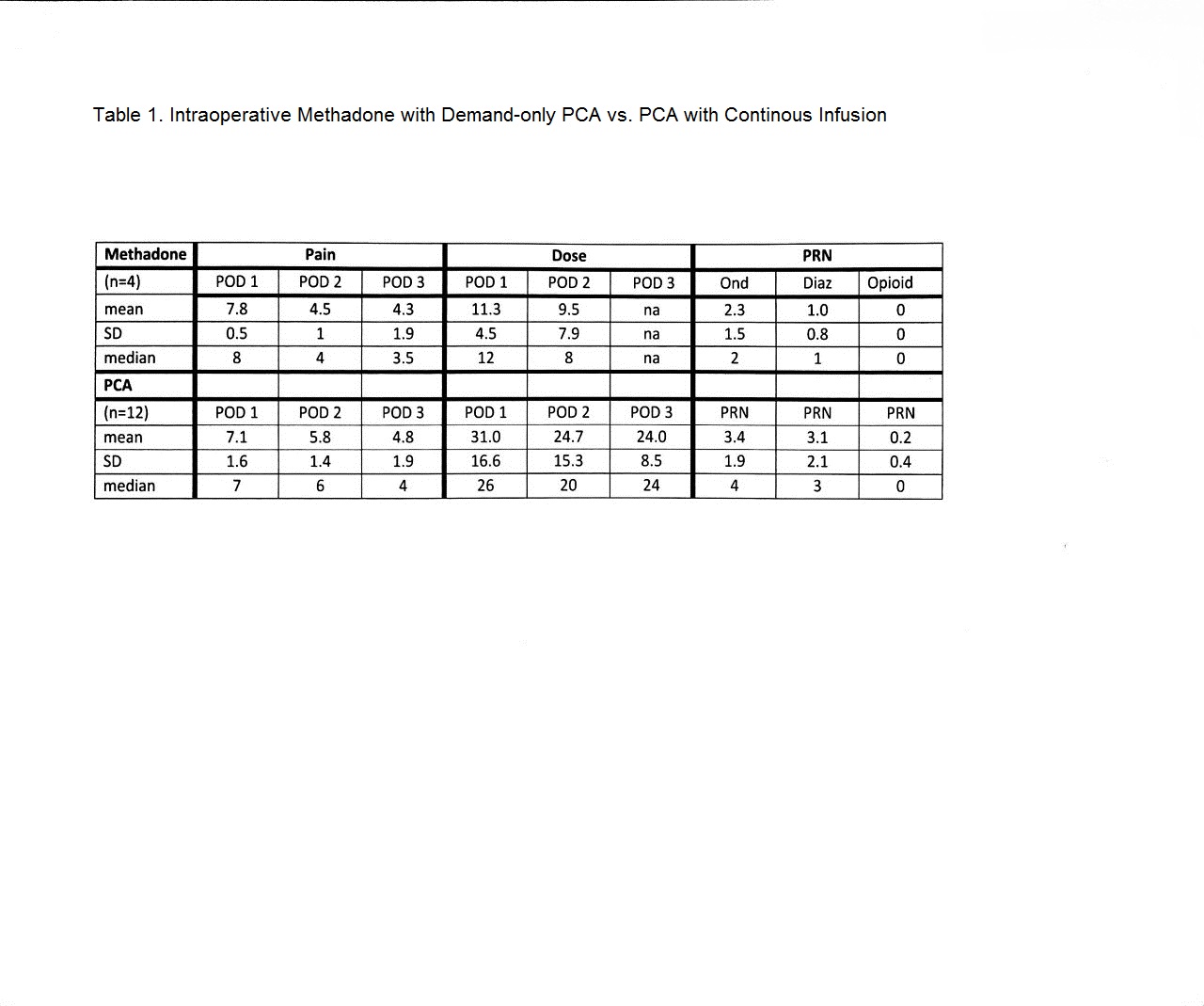
RESULTS: Sixteen charts were reviewed; 4 patients received intraoperative methadone and postoperative demand only PCA, and the 12 patients received postoperative PCA-C. PCA opioid was either morphine or hydromorphone, at equipotent per kilogram doses. Comparative data, presented in Table 1, shows that between the 2 groups, maximum daily pain score were similar but the number of demand doses delivered was lower in the patients who received methadone. For all patients who received methadone, PCA was electively discontinued on Postoperative Day #2. There were no significant differences in PRN medication usage between the two groups.
DISCUSSION: In this QI project, there was a reduction in PCA use in patients who received methadone intraoperatively. Intraoperative loading of methadone has been reported to reduce postoperative pain for different surgeries at different doses: MIRPE: 0.1mg/kg, posterior spinal fusions 0.2mg/kg and adult cardiac surgery (0.3mg/kg). A full investigation of methadone 0.2 mg/kg for MIRPE is planned.
REFERENCES:
Ghionzoli et al. A Pain and Anxiety Management in Minimally Invasive Repair of Pectus Excavatum Korean J Pain (2012 Oct); 25: 267-271.
Litz et al. Enhancing recovery after minimally invasive repair of pectus excavatum. Pediatr Surg Int (2017) 33:1123–1129.
Murphy et al. Intraoperative Methadone for the Prevention of Postoperative Pain. Anesthesiology (2015) 122 1112-1122
Singhal et al. Multimodal anesthesia with the addition of methadone is superior to epidural analgesia. J Pediatr Surg (2016) 51: 612-616.
-
 NM-277 Image 1
NM-277 Image 1
Top










