
NM-297
Controlled CHAOS: A case report of undiagnosed congenital high airway obstruction syndrome due to a laryngeal cyst
Cashin J
UCLA, Los Angeles, CA, USA
INTRODUCTION
There are few scenarios more gut-wrenching than an unanticipated difficult airway. Often algorithms disintegrate into chaos. While there are many case reports of pediatric difficult airways, there are scant reports of neonatal difficult airways. In both the literature and the pediatric difficult airway algorithm, a major junction in the difficult pediatric airway algorithm is the ability or inability to ventilate. This was certainly true for this case
CASE:
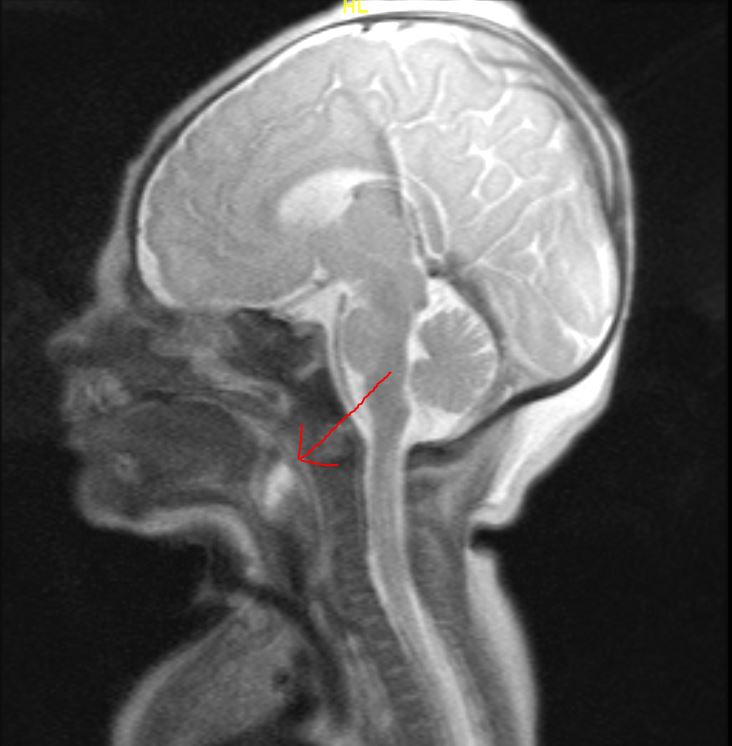
Patient IS was born via NSVD at 39weeks gestational age to a 29 year-old G1P0 mother with GDMA2. Immediately after birth, the patient was noted to be in severe respiratory distress. Intubation was attempted unsuccessfully by multiple providers, revealing a grade 4 view and presence of a mass in the posterior oropharynx. Positive pressure ventilation was possible to maintain hemodynamic stability. Venous blood gas at this time revealed profound mixed metabolic and respiratory acidosis. The decision was made to take the patient to the operative room for tracheostomy. After tracheostomy the patient underwent hypothermia for neuroprotection and was transported to UCLA for higher level of care.
The patient was brought to the OR on day 6 of life for a direct laryngoscopy (DL). Initial DL by the ENT revealed a large non-vascular appearing mass fully obstructing the airway. The mass was lateralized and the epiglottis was visualized. Cyst excision resulted in extravasation of clear fluid, and the mass was partially excised. A second DL revealed a grade 1 view. Pathology was consistent with a saccular cyst. The patient required a second procedure to remove residual cyst. He was ultimately decannulated. Follow-up MRI brain was negative for hypoxic ischemic encephalopathy (HIE).
DISCUSSION
Among congenital laryngeal malformations, cysts are uncommon. Together, vocal fold paralysis and laryngomalacia account for up to 80% of all malformations. The least common malformations include cysts and laryngeal atresia. Overall, laryngeal cysts are routinely diagnosed in adulthood during a workup for an unrelated medical issue. Conversely, laryngeal atresia can present with asphyxia at birth requiring emergent tracheostomy. Notably, congenital laryngeal cysts can also cause marked upper airway obstruction, especially in neonates. Saccular cysts, which are fluid-filled submucosal cysts covered in normal mucous membrane, can cause near total airway obstruction as was the case in our patient. In this case, maintenance of spontaneous ventilation with the addition of supported positive pressure ventilation were lifesaving. If ventilation had not been possible, the outcome could have been devastating. In hindsight proceeding more quickly to tracheostomy may have prevented progressive acidosis and concern for HIE. Ultimately, in cases such as this, the best means of avoiding disaster remains the availability of equipment and staff to perform a tracheostomy.
-
 NM-297 Image 1
NM-297 Image 1
Top










