A New Approach to an Old Technique - Caudal Ultrasound
By Franklin B. Chiao, MD
Assistant Professor of Anesthesiology
Komansky Children’s Center
New York Presbyterian Medical Center
Weill Cornell Medical College
Intro
Caudal block has for many years been a safe technique for providing analgesia in infants. With the recent introduction of ultrasound for regional anesthesia, ultrasound for caudal has become a helpful variation of the traditional palpation based technique. It has been shown that with the palpation based approach, caudal failure rate can be as high as 10-20%(1). With ultrasound guidance, this failure rate decreases. Local anesthesia injection can be seen in many infants and helps to further confirm placement. It can also serve to improve sacral landmark identification in obese children, patient's with difficult anatomy, or for teaching. Ultrasound has been used before for scanning the caudal area in patients with spinal dysraphism.
Anatomy
The focal anatomical area of interest is the sacral anatomy. The sacral cornua surround the sacral hiatus bilaterally. The sacrococcygeal ligament covers the hiatus. These can be palpated on physical exam. Anesthetic placement is through the sacral hiatus. As children age, their posterior spine becomes less cartilaginous and neuraxial imaging is more difficult.
Preparation
Initial preparation is similar to the landmark techniques with the patient in the lateral decubitus (most common) or prone position. The caudal area is cleaned with sterile technique. Next the ultrasound is setup. Since the target depth is shallow, a high frequency probe such as a linear 15-10 MHz probe is prepared and the depth of the screen image is shallow. A cover is placed on the probe in sterile fashion. Traditionally, a 22g needle has been used which is sufficient for the ultrasound procedure. Local anesthetic is also prepared in the usual fashion and at the discretion of the anesthesiologist.
Technique
An attempt to palpate for sacral landmarks can be helpful. The ultrasound probe is placed in a transverse (axial) or longitudinal (sagittal) approach. Gain and depth adjustments to optimize image quality may be performed. It feels easier to start transverse and look for midline anatomy. A "teddy bear ears" image appears on the screen as the hyperechoic sacral cornua are the lobes of the ears (Figure 1 arrows). The sacrococcygeal ligament is also hyperechoic and is a white band between the cornua. In contrast, the sacral hiatus is hypoechoic and beneath the ligament.
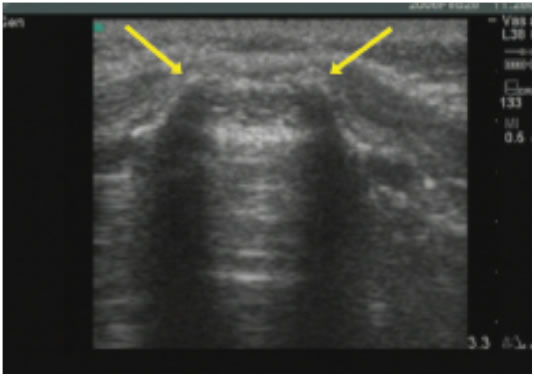
Figure 1- transverse image from Schwartz 2008
A longitudinal midline or paramedian scan reveals additional sacral anatomy including the sacral canal, and posterior surface of the sacrum (Figure 2). In some cases, the cauda equina are visible. While holding the probe in longitudinal fashion as the catheter is advanced in an in-plane technique, the anesthesiologist can see the catheter advance into the caudal space (Figure 3). Injection of local can be seen in many infants but becomes much harder as age increases particularly after one year of age. Although some would describe the use of ultrasound for caudal as an advanced ultrasound technique, it seems that even colleagues with minimal experience have learned quickly. The additional time to setup the probe and to scan is a consideration, but should be weighed against the improved confidence in finding the relevant anatomy and higher placement success rate.
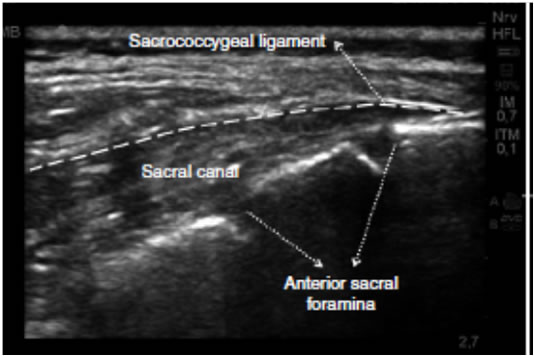
Figure 2- Longitudinal view from Najman 2011
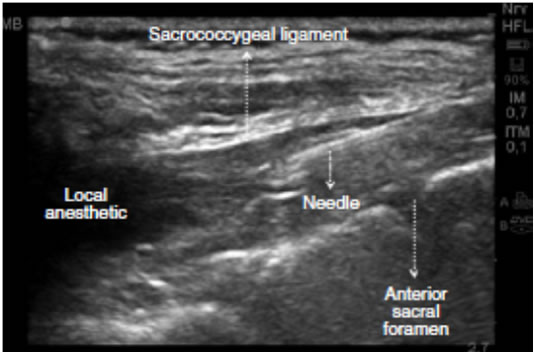
Figure 3- Longitudinal view with needle visible from Najman 2011
Conclusion
Caudal anatomy can be identified with ultrasound. With the increased access to ultrasound machines, this is a reasonable addition to improving caudal block success rate. Furthermore, the sacral canal can also be identified with ultrasound in younger infants.
References:
- Dalens B, Hasnaoui A. Caudal anesthesia in pediatric surgery: success rate and adverse effects in 750 consecutive patients. Anesth Analg. 1989 68:83-89 Schwartz D1, Raghunathan K, Dunn S, Connelly NR. Ultrasonography and pediatric caudals. Anesth Analg. 2008 106:97-99
- Najman IE1, Frederico TN, Segurado AV, Kimachi PP. Caudal epidural anesthesia: an anesthetic technique exclusive for pediatric use? Is it possible to use it in adults? What is the role of the ultrasound in this context?. Rev Bras Anestesiol. 2011 61:95-109
![]()